|
You are a paddle raft guide on the Salmon River during high water; the air temperature is 72º F and water temperature is 54º F. You are at the put-in waiting for your clients to arrive. The bus pulls up and the clients disembark in wetsuits and life-jackets and move to their assigned guides for a safety talk. Your clients all know one another, joined the trip after seeing a brochure during a planned holiday to celebrate the 70th birthdays of two group members, and have never been whitewater rafting before. The entire group is retired, in their late 60s or early 70s, and appear to be in good health for their age. After your safety talk, two of the men, Paul and Andrew, tell you they are each taking a beta blocker for a heart condition. The day run from Riggins to Lucille contains two large rapids where a paddle raft guide needs to rely on the strength and ability of the clients to get the raft to the right place in each rapid; the raft could flip or throw one or more clients in the rapid if in the wrong spot. What are your concerns, if any, and what should you do? Click here to find out. Don't know where to begin or what to do? Take one of our wilderness medicine courses. Guides and expedition leaders should consider taking our Wilderness First Responder course.
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available.
0 Comments
Introduction Heat is part of summer; some people love it...and others, not so much. Regardless of which camp you reside in, excessive heat, typically combined with exercise, can cause a number of potentially fatal, and certainly uncomfortable, heat and heat-related problems (e.g., dehydration, heat exhaustion, heat stroke, exertional rhabodomyolysis, and exercise-associated–exertional–hyponatremia; refer to the graphic below to see the relationship between the major heat related problems). 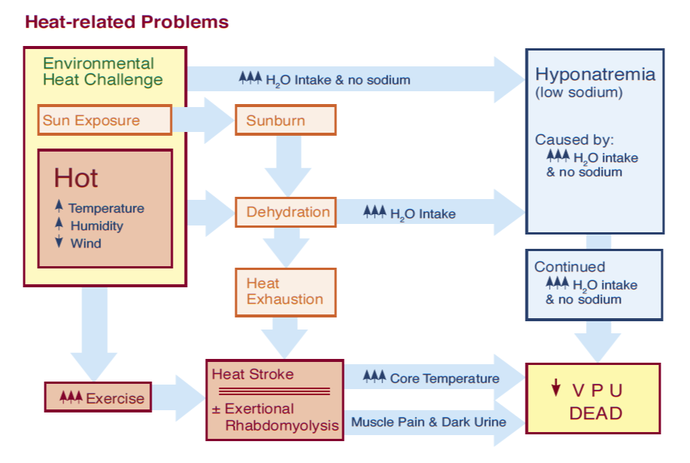 Prevention and proper hydration is key to avoiding all heat-related illnesses, and the cornerstone of prevention is to allow your body enough time to acclimatize to a new heat challenge. With that said, the drugs listed below can predispose outdoor adventurers to a variety of heat illnesses and heat-related problems. Check to see if your friends, clients, or students are taking any of them before venturing into the outdoors this summer when it's hot outside. (A printed drug guide, app, or website will help you understand the side effects, contraindications, and administration guidelines for most drugs.) If you find that they are taking a drug that predisposes them to a heat illness:
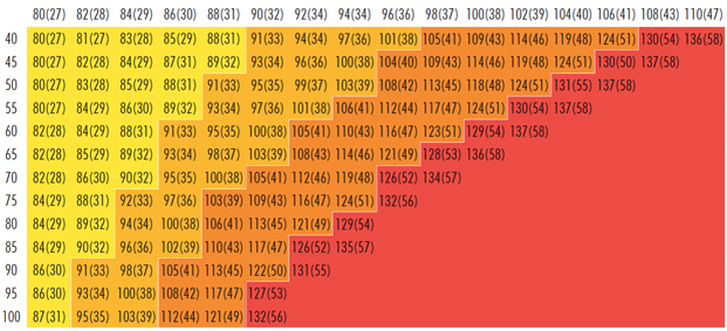  The National Weather Service (NWS) heat index values in the above chart are for shaded, light-wind conditions. Exposure to full sunlight can increase heat index values by up to 15° F; and, strong winds, particularly with very hot, dry air, can be extremely hazardous Anticholinergics Anticholinergic drugs block the transmission of the neurotransmitter acetylcholine in the central and peripheral nervous system responsible for the autonomic control of the smooth muscles primarily in the gastrointestinal (GI) tract, the genitourinary tract, and the lungs. They are used to treat:
Antihistamines Antihistamines block histamine receptor sites in mast cells and basophils, smooth muscle, the lining of lymph and blood vessels, and histamine-releasing neurons in the brain. There are two subcategories of antihistamines: H1 and H2; both are used to treat allergies. H2 antihistamines, because they bind to histamine receptors in the gut, are also used to treat peptic ulcers and acid reflux and H1 antihistamines, because they cross the blood-brain barrier and bind to histamine receptors in the hypothalamus, may be used to treat insomnia in adults and motion sickness. Similar to anticholinergic drugs, antihistamines inhibit sweating and predispose people to both heat exhaustion and heat stroke. Opioids Opioids—including their semi-synthetic and synthetic derivatives—are used to manage both acute and, to a lesser extent, chronic pain; strong opioids are highly addictive. Codeine, a weak opioid, is commonly used in over-the-counter (OTC) pain medications and cough suppressants. Loperamide, an opioid that cannot cross the blood-brain barrier acts on the large intestine to suppress diarrhea. All opioids decrease blood flow to the skin and predispose people to heat stroke. Pseudoephedrine Pseudoephedrine is a stimulant that acts on the smooth muscle lining the blood vessels and bronchi causing them to constrict; it is used to treat sinus and nasal congestion and promote drainage of the sinuses and the Eustachian tubes. Because it's a vasoconstrictor, pseudoephedrine decreases blood flow to the skin and predisposes people to heat exhaustion and heat stroke. Diuretics Prescription diuretics are first-line drugs used to treat high blood pressure. Along with caffeine, prescription diuretics promote dehydration via excessive urination and, through that route, predispose people to heat exhaustion, heat stroke, and—because they deplete the body of sodium—hyponatremia. Selective Serotonin Reuptake Inhibitors (SSRIs) SSRIs are a class of drugs primarily used to treat depression and anxiety disorders but may also be used to treat post traumatic stress disorders (PTSD). The exact therapeutic mechanism is unknown and the side effects of SSRIs may outweigh their benefit. All SSRIs can cause dehydration, which, in turn, can lead to more serious heat illnesses. Ibuprofen & Naproxen Both ibuprofen & naproxen belong to a family of drugs called non-steroidal anti-inflammatory drugs (NSAID) that are commonly carried in first aid kits to treat pain or reduce a fever. While neither drug predisposes people to a heat illness, CAUTION is advised as they can cause kidney damage in the presence of dehydration. Antipsychotics Antipsychotics block receptor sites in the brain's dopamine pathways and are used to treat schizophrenia and bipolar disorders, and combined with antidepressants to treat depression in the short term. Unfortunately, they can inhibit the body’s ability to regulate temperature and predispose people to heat stroke. Beta Blockers Beta receptors are found in the smooth muscle cells of arteries, bronchi, kidneys, and the heart. When stimulated by epinephrine and other stress hormones, they cause a sympathetic stress response that, among other things, increases heart rate and blood pressure. Beta blockers weaken the stress response and are primarily used to manage abnormal heart rhythms and prevent a second heart attack. (They may also be used to treat high blood pressure but are not as effective as diuretics.) They reduce blood flow to the skin and and predispose people to heat stroke. Calcium Channel Blockers Calcium channel blockers disrupt the movement of calcium through cell membranes and are used to treat high blood pressure. They help increase the elasticity of the wall of large blood vessels allowing them to stretch and expand. In this way they also reduce chest pain caused by angina pectoris. They are more effective than beta blockers but have more side effects. Similar to beta blockers, they also reduce blood flow to the skin and predispose people to heat stroke. Ephedrine, Amphetamines, & Cocaine Ephedrine, amphetamines, and cocaine are central nervous system stimulants. Ephedrine is used as a stimulant, appetite suppressant (currently banned in the United States), concentration aid, and decongestant; it works by increasing the activity of norepinephrine. Amphetamines are used to treat attention deficit hyperactivity disorder (ADHD) and narcolepsy. Cocaine is made from the leaves of the coca shrub with no current medicinal use; it is primarily used as a recreational drug...as are many amphetamines. Ephedrine, amphetamines, and cocaine increase internal body temperature, constrict blood vessels, and predispose people to heat exhaustion and heat stroke. Tricyclic Antidepressants Tricyclic Antidepressants (TCAs), as the name implies, are primarily used in the treatment of mood disorders; they are also used to treat chronic neuropathic pain and as migraine prophylaxis (but will not treat a migraine attack). TCAs also decrease sweating and inhibit the body’s ability to regulate temperature and predispose people to heat exhaustion and heat stroke. ACE Inhibitors ACE inhibitors are primarily used to treat heart and kidney problems. They block the production of enzymes that cause vasoconstriction and permit blood vessels to relax (dilate) reducing both blood and kidney pressure. ACE inhibitors may cause increased sweating in some patients, which may quickly lead to dehydration in a heat challenge, and by that route predispose people to heat exhaustion and heat stroke. Lithium Lithium is a mood stabilizer used to treat bipolar disorders and is primarily cleared via urine. While lithium does not predispose people to any heat illness, if a client taking lithium loses a lot of fluid quickly through sweating—which, depending on the individual can easily occur in a moderate or severe heat challenge—their lithium level may quickly rise to toxic levels.
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available.
You are part of a search and rescue team looking for two lost climbers on Mount Washington. The search is entering its third day when, with the help of rescue dogs, the climbers are both located in a snow cave that was hidden from view by a fresh layer of snow from a storm the previous night. The climbers are both unresponsive with no pulse or respirations. They are huddled together and wearing parkas. One of the climbers, James Standing, has an angulated lower right leg; the other climber, Asa Cochran, appears to be uninjured. The average temperatures on the mountain ranged from a daytime high of 16º F to a nighttime low of -4º F. The day is clear with a light wind, and a helicopter is on standby at the Appalachian Mountain Club lodge on Route 2 at the base of the mountain. You are in communication with the lodge and Incident Command via satellite phone. What is wrong with James and Asa and what should you do? Click here to find out. Don't know where to begin or what to do? Take one of our wilderness medicine courses. Guides and expedition leaders should consider taking our Wilderness First Responder course.
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available.
Don't know where to begin or what to do? Take one of our wilderness medicine courses. Guides and expedition leaders should consider taking our Wilderness First Responder course.
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available. Introduction Trip medical forms can reduce program liability and help administrators and field staff prevent injuries and illnesses. In most cases, prevention is accomplished through appropriate screening of participants and modifying the structure of a trip by adjusting the trip’s activities and routes to accommodate individual medical conditions or concerns. The type and format of a trip medical form affects the quality of information received and the ability of program administrators and field staff to prevent and treat injuries and illness in the field. Why require medical forms for trips?
How is client medical information collected? Medical information may be collected orally from the client or via a written medical form. Collection is more effective if all involved—client, guide/instructor, healthcare provider, etc.—know why the information is important and how it will be used. There are two basic types of written medical forms: Those completed by a health care professional (physician, PA, or nurse), and those completed by the client (self-reporting). Medical forms completed by a health care professional—especially if they are the client's personal physician—tend to be the most accurate. Those completed by professionals with little or no previous knowledge of the client—college or university clinics, for example—can miss some conditions if the providers rely heavily on patient self-reporting. Self-reporting may be oral or written. Oral self-reporting typically takes place the day of the trip, often as clients are ready to embark on the trip. The accuracy of oral self-reporting is questionable as it's easy for clients to forget something important or simply not mention it for fear they will not be permitted to go on the trip. Clearly written self-reporting forms are better than oral self-reports. Written forms—regardless of whether completed by a healthcare professional or by the client—tend to be more effective when a combination of check boxes and open-ended questions are used. For example, here's a question with Yes/No checkbox followed by a series of open-ended questions asking for more information: "Are you taking any prescription medications?" (Yes/No) "If you answered "yes" to the above question please:
If client medical information is so important, why don't all outdoor programs collect it?
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available.
IntroductionThe Act of Drowning Contrary to how it is often depicted in movies, the act of drowning often goes unnoticed. There appear to be three separate actions or body positions people adopt when confronted with the possibility of drowning. Depending on their swimming ability, injuries, or illnesses, some will progress through all three of these stages, while others will not.
Drowning In drowning, the victim is submerged under or immersed in water and requires rescue or assistance; not all drowning victims are unresponsive during their rescue; they may be awake, voice responsive, or pain responsive. Drowning is a process with three possible outcomes:
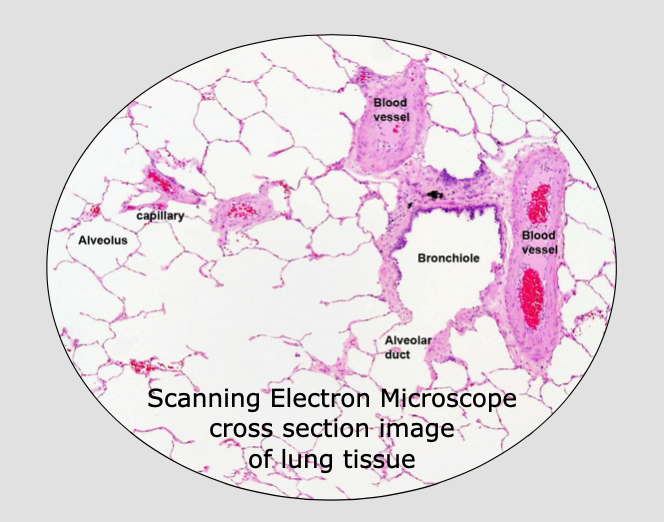
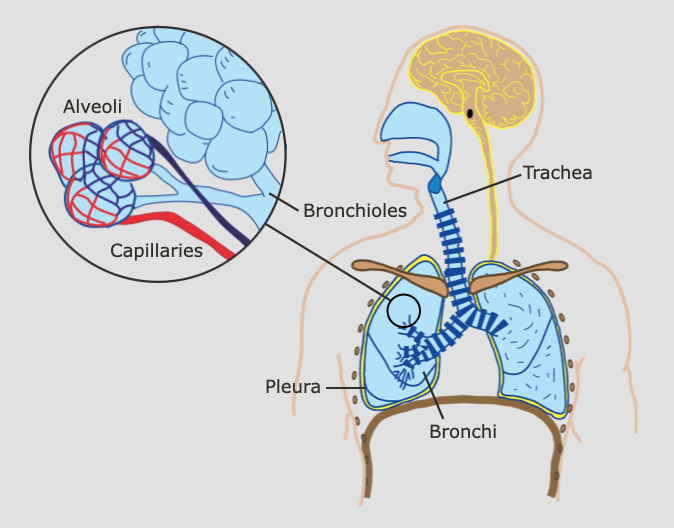
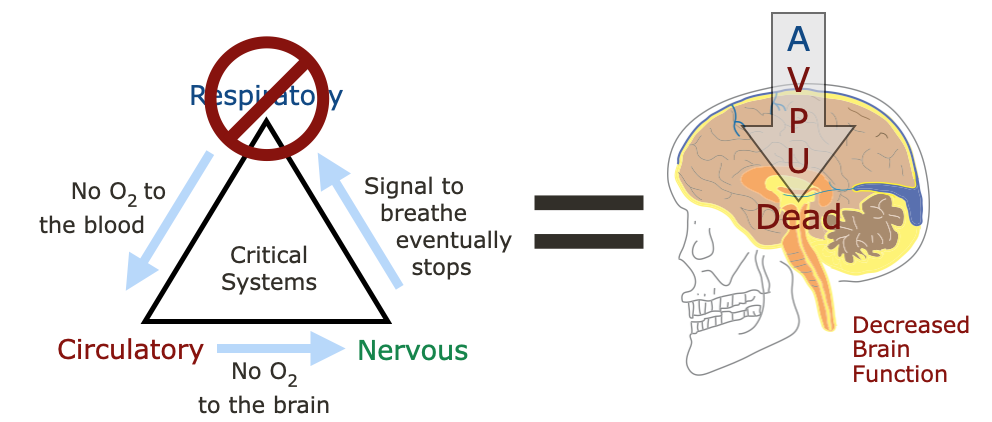 Ultimately, drowning patients die from a lack of oxygen. Our lungs cannot extract oxygen from water. Anatomy & Physiology
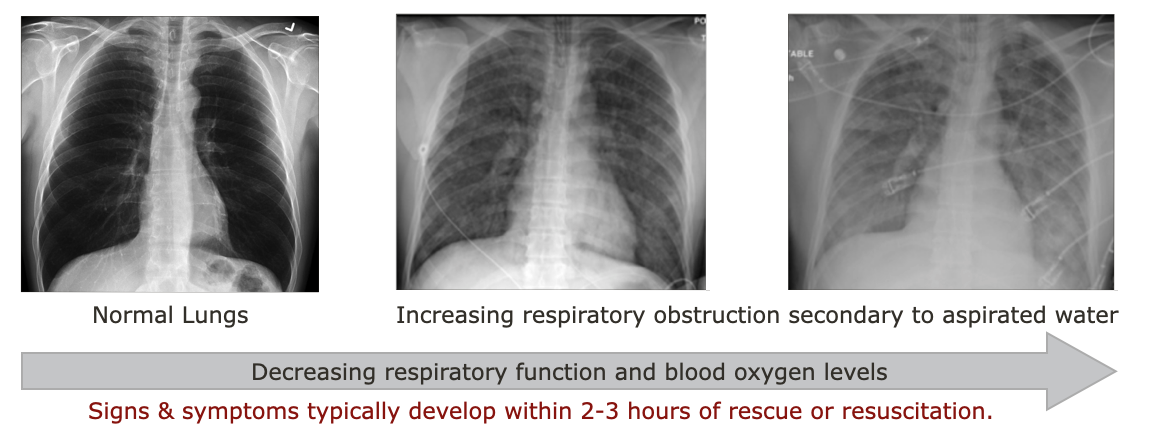
Pathophysiology Contrary to popular belief, very little water enters the lungs of most drowning victims:
Why so little? When water enters the drowning victim's mouth and nose, their epiglottis immediately closes and covers the trachea and they reflexively swallow. As a result, literally liters of water has been found in the stomachs of fatal drowning victims. This reflexive protection typically remains intact until the patient becomes runs out of oxygen and gasps for air or becomes unresponsive, and even then, little water actually enters the victim's lungs. Unfortunately, it doesn't take much aspirated water to cause problems and interfere with the gas exchange in the alveoli. Patients who have a pulse and are breathing after rescue or resuscitation, may develop respiratory complications severe enough to cause death minutes to hours after the incident if they aspirate enough water.
Basic Life Support Assessment & Treatment
Follow up Assessment, Treatment, & Evacuation
Interested in learning more about wilderness medicine? Take one of our wilderness medicine courses. Guides and expedition leaders should consider taking our Wilderness First Responder course.
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available. Introduction Stress is inherent in outdoor trips and activities. People can often adapt to mild stress and return to their baseline relatively quickly; however, chronic, moderate, or severe stress may overwhelm an individual’s coping mechanisms and result in a mental health problem. S/Sx include increasing inability to cope with the challenges of the trip, activity, or group. The graphic below depicts the different levels of distress and their associated evacuation levels with respect to a mental health event 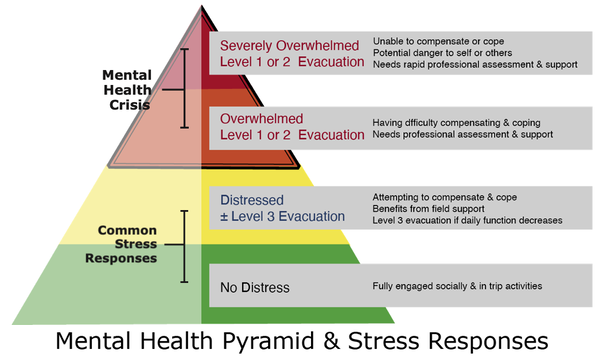 To help avoid a mental health crisis on expeditions or trips, it is critical to identify and evaluate an individual’s distress early. Check in with the group or individuals daily or after potentially stressful events as part of the expedition culture and stress management. Consider using colors as a tool to help group members self-identify their current stress level. Green = no distress Yellow = distressed and actively compensating or coping Orange = overwhelmed having difficulty compensating or coping Red = severely overwhelmed and no longer compensating or coping People who self-identify as distressed, overwhelmed, or severely overwhelmed need support and should be encouraged to seek out and speak with staff or the trip leaders privately. Similarly, if staff or trip leaders observe behaviors that indicate a participant may be in distress or crisis, they should speak privately with the individual. Depending on the participant’s story and presenting S/Sx, they may elect to support them in the field or begin an evacuation. S/Sx of Potential Behavioral & Psychological Distress
Support Guidelines Participants who are in distress but actively compensating (yellow) may remain in the field if supported and their daily functioning monitored. Support participants by:
Evacuation Guidelines
Don't know where to begin or what to do? Take one of our wilderness medicine courses. Guides and expedition leaders should consider taking our Wilderness First Responder course.
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available. (What are they and should I join one?) With the worldwide increase in natural disasters, wilderness medicine graduates are uniquely poised to help their neighbors in the event of a local disaster. Communities in all 50 states have organized Community Emergency Response Teams (CERT). CERT members are volunteers, and teams are structured so that local managers have the flexibility to adapt the program and their training to the specific needs of their community. The concept originated with the Los Angeles City Fire Department in 1985 and went national through the Federal Emergency Management Agency (FEMA) in 1993. Contact your local fire, police, or sheriff department for more information or visit the CERT website.
You are part of a search and rescue team looking for survivors a day after a devastating wildfire passed through your town. It's been raining non-stop for the past 12 hours making your task more difficult. Mud slides have closed a number of roads slowing evacuation and exacerbating the entire situation. As you walk the shoreline of one of the nearby lakes, you see someone waving in an attempt to attract your attention from an island roughly half a mile from shore. Borrowing an aluminum rowboat from one of the burned-out cabins, you and your partner row to the island. Once there, you are confronted by a 32-year-old mother who is wet, shivering, and seeking help for her six-year-old daughter, Jolene. Jolene is huddled in a leaky, make-shift shelter, swathed in a wet blanket. She responds to your questions with short, mumbled phrases. Her mother, Trish, reports that they fled the fire by swimming to the island yesterday, that both she and Jolene are uninjured, and that they have had no food since early yesterday. Trish said she had to swim with Jolene most of the way. The water temperature is in the mid-60s F. It's now 4:30 pm and the rain is not letting up. You are in communication with Incident Command via satellite phone. What is wrong with Jolene and what should you do? Click here to find out. Don't know where to begin or what to do? Take one of our wilderness medicine courses. Guides and expedition leaders should consider taking our Wilderness First Responder course.
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available. (What to do when someone dies in the backcountry.) Deaths in the backcountry are rare, exactly how rare is up for debate. Much depends on how you define backcountry and where you get your numbers (outside of the National Park Service, accurate statistics are hard to find). That said, a few hundred people appear to die each year while recreating in the outdoors. Given the number of people who play outside annually, statistically, death is pretty rare. While the order often changes annually, the top ten causes of death in the backcountry appear to be:
So what should I do if I'm with a person who is dying? There is no single answer that applies to all people other than support their process to the best of your ability. For many, this means holding their hand and simply being present. For some, it may include praying with or for them. If the person is awake, it may mean taking notes to share with relatives and friends. The specifics vary from individual to individual. How do I know when a person is dead? They will not have any signs of life: no pulse at their carotid artery, no chest rise, and no air coming from their mouth or nose. Over time their body will cool until it reaches the ambient air temperature and rigor mortis and liver mortis will set in. Rigor Mortis: When energy is no longer being produced, muscles contract and stiffen beginning with the small muscles of the face, neck, arms, and shoulders and gradually encompassing larger muscles until the person's body is completely stiff. Rigor is typically fully set within eight hours and remains in place for roughly eighteen hours before reversing itself to pre-rigor status, starting with the large muscles. Liver Mortis: When a person's blood stops circulating after death, gravity causes the red blood cells to settle leaving dark "bruising" in areas of the patient's body that are in contact with the ground. The process begins roughly thirty minutes after death and is fixed after approximately six hours. What should I do after a person is dead? Keep in mind that your first priority is yourself and the living members of your party. Make sure everyone is safe. Then, if possible, note the GPS coordinates of the body's location and notify the local authorities via radio, cell phone, satellite phone, or other communication device and follow their instructions. If the dead person was your patient, complete a SOAP note. If they were a client or student, also complete your program's accident/incident report form. Take pictures of the site and body, especially if the mechanism was trauma, and do your best to preserve the scene for the authorities; most states prohibit moving a dead body from the scene of the accident without the authority of the coroner. Of course, some scenes cannot be preserved due to weather or terrain. If you can't contact and receive direction from local authorities and find you must leave the scene, your photos become evidence and part of any subsequent investigation. If you decide to leave the scene and the body, do your best to protect the body from scavengers and clearly mark its location both visually and on a map. Although rare, some expeditions have decided to transport the body of the deceased out of the backcountry. Treat the body with respect and be sensitive to the cultural mores of the deceased and those around you. |
Categories
All
Our public YouTube channel has educational and reference videos for many of the skills taught during our courses. Check it out!
|


 RSS Feed
RSS Feed