|
You are the trip leader for a two-week high school snowshoe trip in the Adirondack mountains of New York state. It's day four. There was six inches of new snow on the forest road at the beginning of the trip. Last night it snowed three feet and it is still snowing hard. Looking closely at your map you realize that your original route crosses a few potential avalanche paths. After talking it over with your co-leader and considering the ever-increasing snowfall, you decide to reverse your route and head back. You have no satellite or cell phone reception during the storm. After a day of struggling through the deepening snow, everyone is exhausted and wet from either sweat or snow when you reach your evening camp. You notice that two 16 year-old girls are particularly tired and shivering. What are your concerns and what should you do? Click here to find out. Don't know where to begin or what to do? Take one of our wilderness medicine courses. Guides and expedition leaders should consider taking our Wilderness First Responder course.
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available.
0 Comments
You are a trip leader on a five-day winter break backpacking trip in Linville Gorge, NC. It's day three of the trip when the gorge is hit unexpectedly with 14 hours of freezing rain. The rocks, trails, and trees are covered with an inch of ice; numerous trees have fallen, leaving the trails littered with trees and tree limbs, further increasing the difficulty of foot travel. You are camped at the bottom of the gorge and scheduled to be picked up at 10 AM on the fifth day. To reach the pick-up at the scheduled time, you need to hike most, if not all, of the day. What are your concerns and what should you do? Click here to find out. Don't know where to begin or what to do? Take one of our wilderness medicine courses. Guides and expedition leaders should consider taking our Wilderness First Responder course.
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available. Pathophysiology Numerous types of fungi live on and in our bodies without causing harm; they are held in check by competing bacteria and our immune system. Disease-causing fungi can be divided into two groups: filamentous fungi and yeasts. Filamentous fungi are made up of branching threads known as hyphae; yeasts are single-celled organisms. The most common fungal infections are superficial and caused by Tinea, a filamentous fungi and Candida albicans, a yeast. Heat, humidity, immunocompromised states, long term antibiotic use, diabetes, and steroid therapy predispose people to both types of fungal infections. Fungal infections are more common in the summer and exerted by wearing synthetic clothing and sweating. Tinia Infections Tinea infections are caused by a group of fungi (ringworm) that live on keratinous structures and invade dead layers of the host's skin, hair, and nails; the transmission routes are direct contact with an infected person or animal or with contaminated soil. Clinically, tinea infections are classified according to the body region involved/infected: tinea capitis (scalp), tinea corporis and versicolor (trunk and extremities), tinea manuum and tinea pedis (palms, soles, and interdigital webs), tinea cruris (groin), tinea barbae (beard area and neck), tinea faciale (face), and tinea unguium (nails). Candida Albicans (Yeast) Infections Candida albicans skin infections may closely mimic tinea crurisare but are usually moister, more inflammatory, and associated with satellite macules, pustules, and scales. Unlike Tinea, Candida may also infect the mucus membranes of the mouth, vagina, penis, and eye. These infections are red, itchy, moist and often associated with a yeasty odor and a white cheese-like discharge. Most mucosal infections result from long-term antibiotic use. Prevention
Assessment
 Treatment
Don't know where to begin or what to do? Take one of our wilderness medicine courses. Guides and expedition leaders should consider taking our Wilderness First Responder course.
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available. A 35 year-old man hits a tree while skiing out of bounds. Bill is awake, alert, and reliable but fails your focused spine assessment due to cervical pain (8) and tenderness with no neurological deficit. Ski patrol is available to assist with transport via a Cascade toboggan and snow mobile. Estimated arrival to scene is 45 minutes and transport to an ambulance is expected to take another two hours with arrival at a local hospital in another hour. Total response and transport time to the hospital is estimated at roughly ± 4 hours. The outside temperature is 22º F and the patient has additional thermal layers in his pack. His remaining injuries are compatible with self-evacuation. Should you keep him quite and immobile and wait for help or begin a self-evacuation. Click here to find out. Click here to read a blog article on current spine management guidelines. Don't know where to begin or what to do? Take one of our wilderness medicine courses. Guides and expedition leaders should consider taking our Wilderness First Responder course.
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available. Geoff Jones, 52, is swept away in a medium sized soft snow avalanche while skiing in the backcountry. He travels approximately 400 feet and is recovered partially buried. He is awake, alert, and reliable with cervical spine pain and tenderness. He reports a tingling, electric-like pain in his right arm when his neck moves; he cannot distinguish between pinprick pain and light touch on his right hand; and, there is noticeable weakness on his right side when executing the motor exams on his hands. His remaining injuries are compatible with self-evacuation. There is no cell service and no one in the group is carrying bivy equipment with them or on their snowmobiles six miles away. Help is roughly twelve hours away. It's 3:30 pm in mid-January; sunset is within the next hour. The current air temperature is 21º F. Clouds are moving in, the wind is picking up, and it looks like it's going to snow. Should you keep Geoff quiet and immobile and go for help or begin a self-evacuation? Click here for answers. Click here to read a blog article on current spine management guidelines.
Don't know where to begin or what to do? Take one of our wilderness medicine courses. Guides and expedition leaders should consider taking our Wilderness First Responder course. Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available. Fleas, mosquitoes, lice, assassin bugs, sand flies, chiggers, ticks and other biting insects may be carriers of an infectious disease. With the advent of global warming, insects and insect-borne infectious diseases are spreading to new areas. To protect yourself against contracting an insect-borne infectious disease, the Centers for Disease Control and Prevention (CDC) recommends using the following insect repellents and insecticides; they have been shown to be safe and effective, even in pregnant and breastfeeding women. Clothing, tents, and mosquito netting are ideal for first order of protection and sleeping, especially when saturated with Permethrin (which kills insects on contact). To protect against chiggers and ticks, wear light-colored or white long pants, long-sleeved shirts, and socks so ticks can be more easily seen; pull socks over pant cuffs. Wear a hat and place petroleum jelly around hairline to keep ticks from crawling into hair (where they will be very difficult to find). Do a thorough tick check each morning & evening before entering and leaving your tent. The CDC does not recommend other insect repellents and products as they have not been shown to be effective despite manufacturers claims. These include natural plant oils, (such as citronella oil, cedar oil, geranium oil (or geraniol), and lemongrass oil), repellents containing vitamin B1 or garlic, and wristbands and ultrasonic devices. Application
DEET
Picaridin
IR3535
Lemon Eucalyptus Oil
Permethrin
Interested in learning first aid? Take one of our wilderness medicine courses. Guides and expedition leaders should consider taking our Wilderness First Responder course.
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available. You are leading a week-long backpacking trip for a local high school. During the night a cold front with high winds passed through breaking tree limbs and blowing down trees. A six-inch limb split off an overhead tree and landed on a student tent, hitting one of the students a glancing blow on his head while in his sleeping bag. When questioned, James said the storm had just woken him up when something hit the tent, collapsed it, and hit him in the head through his sleeping bag. The commotion woke his tent mate and together they managed to push the branch off the tent. They came to get you because James said he had a headache and a big lump on his head. Other than the lump and a headache (3), James says he feels okay. He has no spine pain or mid-line spinal tenderness, normal motor and sensory exams on his hands and feet, and no tingling or electric shooting pain in his arms or legs. His skull feels intact beneath the swelling. What is wrong with James and what should you do? Click here to find out. Don't know where to begin or what to do? Take one of our wilderness medicine courses. Guides and expedition leaders should consider taking our Wilderness First Responder course.
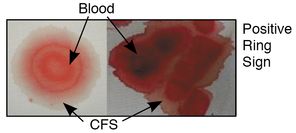
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available. You and your climbing partner are six pitches up on Goat Wall in Mazama, WA when a sudden lightning storm moves in with heavy rain and lightning. Abandoning the climb you begin to simultaneously rappell off (an advanced—and somewhat risky—climbing technique where two climbers rappel at the same time on the same rope counterbalancing one another). On the last rappell, you neglected to tie a knot on your side of the rope and misjudged the distance to the ground, and rappelled of the end of the rope a few feet above the ground. Unfortunately, your climbing partner, Jessie was roughly 20 feet above you when you fell. With the loss of your counterbalanced weight, the rope pulled through the anchor and Jessie fell to the ground landing on her right side and head in the talus. When you reach her, Jessie is unresponsive and bleeding from her nose and ears; some of the fluid appears to be a light yellow and her helmet is cracked. A quick physical exam reveals a soft spot on her skull behind her right ear and crepitus in multiple ribs on her right side. Her pulse rate is 168 and regular; her respiratory rate is 26 and slightly irregular; her skin is pale. What is wrong with Jessie and what should you do? Click here to find out. Don't know where to begin or what to do? Take one of our wilderness medicine courses. Guides and expedition leaders should consider taking our Wilderness First Responder course.
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available. While paddling a Class V section on the Wind River in WA, a 35 year-old intermediate kayaker turned over in a rocky rapid. While upside down, Jamie hit his face and head against a boulder before being scraped out of his boat. He was rescued by his friends unresponsive and with a pulse, but not breathing. He started breathing spontaneously after one of his friends delivered a few rescue breaths. Five minutes later he awakened with a severe headache (7) and no memory of the event. Jamie's neck is stiff and painful (4) with mid-line spinal tenderness at C-3 and a tingling, electric-like pain shooting down his right arm whenever he moves his head. He appears somewhat stunned or dazed and reports numbness in his upper lip and gums and difficulty breathing through his nose. His nose is both painful (4) and tender. He is able to stand but has difficulty with his balance and walking. What is wrong with Jamie and what should you do? Click here to find out. Don't know where to begin or what to do? Take one of our wilderness medicine courses. Guides and expedition leaders should consider taking our Wilderness First Responder course.
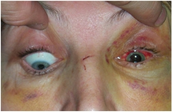
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available. Similar to patients with skull fractures, patients with an orbital, zygomatic (cheek), nasal, maxillary (mid face), or mandibular (jaw) fracture should be evaluated for a concussion, increased ICP, and a cervical spine injury. Patients with nasal, maxillary, and mandibular fractures may present with or develop airway management problems. Orbital Fractures Orbital Fracture S/Sx
Zygomatic (cheek) Fractures Zygomatic Fracture S/Sx
Nasal Fractures Nasal Fracture S/Sx
 Maxillary (mid face) Fracture Maxillary Fracture S/Sx
Mandibular (jaw) Fracture Mandibular Fracture S/Sx
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available.
|
Categories
All
Our public YouTube channel has educational and reference videos for many of the skills taught during our courses. Check it out!
|


 RSS Feed
RSS Feed