|
In combination with our patient assessment system and field handbook, we use SOAP notes to help teach students how to assess and treat patients. They quickly see the benefit in a well-designed SOAP note, especially for complex problems; however, they often question if a SOAP note should be used for every patient? After all they take time to complete (and everyone hates paperwork, particularly if it's seen as unnecessary). So...what's necessary and what isn't? Sometimes the answer is obvious: The problem is serious and/or complex and a SOAP note is necessary. But what about minor problems, for example: blisters, strains and sprains, cuts, etc.; and problems that may, or may not, develop into something more serious, like hymenoptera stings that may progress to anaphylaxis, a blow to the head that may turn out to be a mild concussion, or a drowning patient who was awake throughout their rescue but coughing, etc. These are not so obvious, usually because they don't require an evacuation at the moment...but could in the future. What about them? There are a couple of ways to proceed; both are valid:
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available.
Download a free pdf copy of our 2018 SOAP note for you personal or institutional use; print on 8.5 x 14 legal paper and fold into thirds. Many not be used to teach © 2018 WMTC.
0 Comments
Human health is linked to the health of the environment, including its plants and animals (yes, insects are classified as animals: Kingdom Animalia > phylum Arthropoda). Infectious diseases in humans are caused by viruses, bacteria, parasites, or fungi, and transmission is via one of four routes:
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available.
You are holed up in a snow cave waiting out a heavy winter storm at 10,500 feet in the Colorado Rockies. Your sleeping area is raised a few feet above your entrance. You have been cooking outside with your stove sheltered from the wind by strategically placed snow blocks. A ski pole poked through the roof of the cave provides much needed ventilation. To save batteries, you have been using two candle lanterns to provide enough light to read and play cards. After a day, the air inside the cave is slightly stuffy and both you and your partner have a slight headache. What's wrong and what can you do about it? Click here to find out. Don't know where to begin or what to do? Take one of our wilderness medicine courses. Guides and expedition leaders should consider taking our Wilderness First Responder course.
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available. 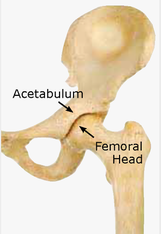 Pathophysiology While posterior hip dislocations are somewhat common in head-on motor vehicle accidents and occasionally occur in elderly people with prosthetic hip joints during a minor slip or fall, they are quite rare in a wilderness environment. Most posterior hip dislocations require a significant traumatic MOI and many patients die from internal injuries to the pelvis, abdomen, chest, and head. Greater than 50% of patients have long-term disability after reduction. The femoral head is highly vascular and may die if not quickly reduced. Posterior hip dislocations are increasing along with the popularity of extreme sports; one study indicated that snowboarders were more likely to suffer a posterior hip dislocation than skiers. The hip joint is a ball-and-socket synovial joint: the ball is the femoral head, and the socket is the acetabulum. The adult hip is quite stable. As such, knee and lower leg injuries are often seen in conjunction with posterior hip dislocations. Due to the potential for significant complications, an attempt should be made to reduce posterior hip dislocations in the field.  Posterior Hip Dislocation Signs & Symptoms
 Interested in anticipating and prevention potential problems in the outdoors? What to be able to take care of your family or friends should something unexpected happen? Take one of our wilderness medicine courses. Guides and expedition leaders should consider taking our Wilderness First Responder course.
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available. While mountain biking down a steep single track your friend catches his front wheel and is thrown forward with his bike. During the fall the handlebars smash into the left side of his chest. Asa has difficulty sitting up and catching his breath, and appears to have injured his left wrist. After assisting him to a sitting position and coaching him to breathe with his abdomen, his respiratory distress appears to resolve. During your physical exam, he reports a sharp pain (7) in the ribs on his lower left chest when he tries to take a deep breath. While his left wrist hurts (4) and has a slightly decreased ROM with good distal CSM, it appears weak: Asa is unable to easily hold and lift a full 1-liter water bottle. His helmet is cracked, he reports feeling a bit woozy, and has a headache (4); the remainder of his physical exam is unremarkable. With abdominal breathing, the pain in his ribs is manageable (3). 20 minutes after his accident his pulse is 94 and regular and his respiratory rate is 22 and remarkably easy; he reports his normal pulse rate is in the mid-60's and he doesn't know his normal respiratory rate. While awake, he still feels a bit "out of it." A focused spine assessment reveals cervical pain and tenderness at C-7 with no shooting pain and normal motor and sensory exams. What is wrong with Asa and what should you do? Click here to find out. Don't know where to begin or what to do? Take one of our wilderness medicine courses. Guides and expedition leaders should consider taking our Wilderness First Responder course.
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available. Contrary to how it is often depicted in movies, the act of drowning often goes unnoticed. There appear to be three separate actions or body positions people adopt when confronted with the possibility of drowning. Depending on their swimming ability, injuries, or illnesses, some will progress through all three of these stages, while others will not.
In a drowning, the victim is submerged under or immersed in water and requires rescue or assistance; not all drowning victims are unresponsive during their rescue and upon recovery, some are awake, voice responsive, or pain responsive. Drowning is a process with three possible outcomes: 1. Death, 2. survival with brain damage, and 3. survival without brain damage. In rare cases, primarily associated with cold water and young children, a few pulseless and apneic victims may also have a complete recovery if rescued within 30-90 minutes—depending on water temperature—and CPR started immediately. These fortunate few will have experienced an immediate shell/core response from core hypothermia or a phenomenon known as the "Mammalian Diving Response" or MDR. Many, but not all, drowning victims will quickly become unresponsive due to a systemic loss of oxygen and minutes later their heart will stop; in most cases, after roughly five more minutes they will suffer permanent brain damage. If not rescued, all unresponsive drowning victims will die. If rescued, the unresponsive patient who still has a pulse (but is not breathing) has a reasonable chance for recovery if rescue breathing is begun immediately. A patient who has no pulse and no respirations may, with immediate CPR, also recover completely, however, mortality is high. Given the potential for core hypothermia or an MDR, start CPR on all pulseless and apneic drowning victims who have been submerged for less than 30 minutes in water warmer than 43ºF (6ºC) or less than 90 minutes in colder water. If a recovery occurs during CPR, it will usually happen within the first few minutes. If pulse and respirations are not forthcoming, continue resuscitation efforts for a full 30 minutes. Click to read an article on cold water immersion. Most drowning victims aspirate very little water because their epiglottis closes and they swallow; the water, sometimes a LOT of water, enters their stomach. The majority of non-fatal drowning patients asperate less than 30 ml (1 oz) of water while fatal drowning patients aspirate 1-2 ml of water per kg of body weight (as found during autopsy). The aspirated water is absorbed into the microvascular bed surrounding the alveoli where it may wash out leading to alveolar collapse and cause an inflammatory response that leads to pulmonary edema (PE). In most cases, the S/Sx of PE will appear within 2-3 hours and non-fatal drowning patients should be monitored for 4-6 hours. Listening with a stethoscope—and occasionally with an ear to the patient's bare chest—will reveal rales, crackling noises that indicate fluid is accumulating in the patient's lungs. Foam in the patient's upper airway—or issuing from their mouth or nose—is the result of plasma (PE) mixing with the displaced surfactant. Decreased water quality increases the likelihood of pulmonary edema and subsequent respiratory infections. While skiing back to your vehicle after a day of touring in the backcountry, your friend skis directly into a 10-inch lodgepole pine at a moderate rate of speed. When you reach her, she is out of breath and struggling to sit up. You carefully assist her to a sitting position and begin your assessment. Jenny's breathing quickly returns to normal. She tells you she got the wind knocked out of her and the right side of her chest is sore (2); on exam, her chest is slightly tender. She did not hit her head. Her pulse and respiratory rates are normal. A focused spine assessment reveals no spine pain, tenderness, or shooting pain and normal motor and sensory exams. Jenny doesn't think she is badly injured and is ready to continue skiing, albeit slightly slower and under better control. What is wrong with Jenny and what should you do? Click here to find out. Don't know where to begin or what to do? Take one of our wilderness medicine courses. Guides and expedition leaders should consider taking our Wilderness First Responder course.
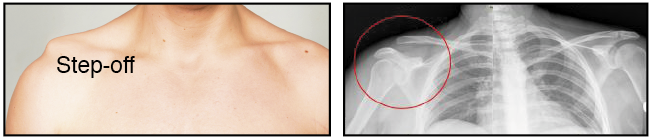
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available. Separated Shoulder A separated shoulder is a dislocation of the acromioclavicular (AC) joint. The MOI is a fall onto the point of the shoulder—the acromion process of the scapula—tearing ligaments and causing the clavicle to ride up and over the acromion; fractures of the acromion and clavicle are possible, but rare. It is a common mountain bike and snow board injury. Separated Shoulder S/Sx
 Separated Shoulder Treatment
 Interested in anticipating and prevention potential problems in the outdoors? What to be able to take care of your family or friends should something unexpected happen? Take one of our wilderness medicine courses. Guides and expedition leaders should consider taking our Wilderness First Responder course.
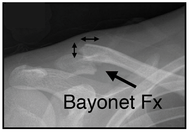
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available. Clavicle Fractures The mechanism of injury is a fall onto an outstretched arm or shoulder, or a direct blow to the clavicle; it is a common mountain bike and snow board injury. Clavicle and first rib fractures typically cause lung damage and respiratory distress. Clavicle Fracture S/Sx
Clavicle Fracture Treatment

Interested in anticipating and prevention potential problems in the outdoors? What to be able to take care of your family or friends should something unexpected happen? Take one of our wilderness medicine courses. Guides and expedition leaders should consider taking our Wilderness First Responder course.
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available. Rib Fractures In most cases, a simple, isolated rib fracture elicits sharp, knife-like pain, and respiratory distress; however, as the patient relaxes and begins to breathe with their diaphragm, the respiratory distress subsides. Depending on the location of the fracture and it's severity, if there are multiple rib fractures especially to the same rib or ribs (flail chest), the patient may present with or develop respiratory distress due to lung damage and/or internal bleeding. Isolated Rib Fracture S/Sx
Interested in anticipating and prevention potential problems in the outdoors? What to be able to take care of your family or friends should something unexpected happen? Take one of our wilderness medicine courses. Guides and expedition leaders should consider taking our Wilderness First Responder course.
Looking for a reliable field reference? Consider consider purchasing one of our print or digital handbooks; our digital handbook apps are available in English, Spanish, and Japanese. Updates are free for life. A digital SOAP note app is also available. |
Categories
All
Our public YouTube channel has educational and reference videos for many of the skills taught during our courses. Check it out!
|
 RSS Feed
RSS Feed